Stenting of High-Risk 99% LMCA Osteal Lesion
Hi everyone
A 70-year-old male presented to the emergency department with shortness of breath and chest pain. ECG revealed ST-T changes and 2D echocardiography showed severe left ventricular (LV) dysfunction. The patient was diagnosed with Coronary Artery Disease (CAD) and Acute Coronary Syndrome (ACS) – Anterior Wall NSTEMI.
Coronary Angiogram (CAG) Findings:
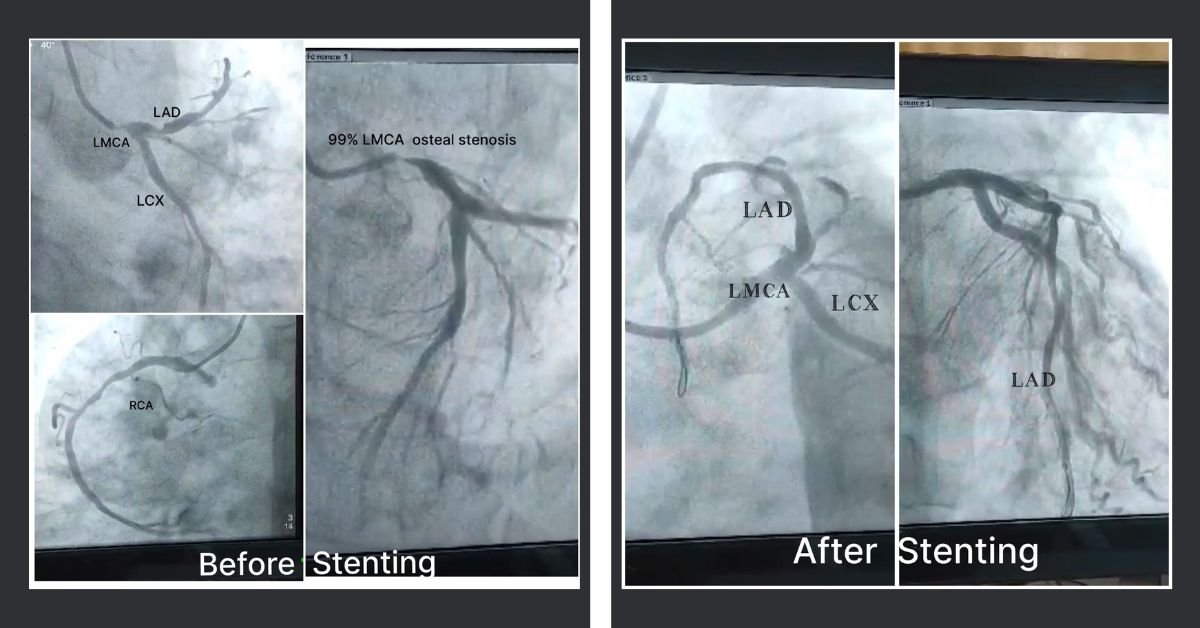
- LMCA: Osteal 99% stenosis
- LAD: Type 3 proximal and mid 80% stenosis
- LCX: Mid LCX 50-60% stenosis
- RCA: Dominant, mid RCA 80% stenosis
- Impression: LM Ostium + Double Vessel Disease (DVD)
- Planned Intervention: Percutaneous Transluminal Coronary Angioplasty (PTCA) of LM Ostium to LAD with Drug-Eluting Stent (DES)
Challenges in This High-Risk Case:
- Unstable patient with severe LV systolic dysfunction
- Risk of ostial occlusion during wiring to LMCA, which could have resulted in immediate cardiac arrest
- Extremely high-risk stenting procedure requiring rapid and precise execution
With God’s blessings, the procedure was completed in a very short time, achieving an excellent final result. This was one of the most critical cases I have performed, requiring timely decision-making and meticulous execution.
A special thanks to the Cath Lab team and Anesthesia team for their timely support in handling this challenging case.

The patient was discharged after four days and returned for follow-up in the OPD with significantly improved LV function. It is truly remarkable how cardiology transforms lives—from being symptomatic and at high risk to becoming completely asymptomatic and thriving.
This case highlights the importance of expertise, timely intervention, and teamwork in managing complex cardiac cases.

